NewAmsterdam Pharma: Resurrecting the CETP Graveyard
Introduction: A Billion-Dollar Bet on a Cursed Drug Class
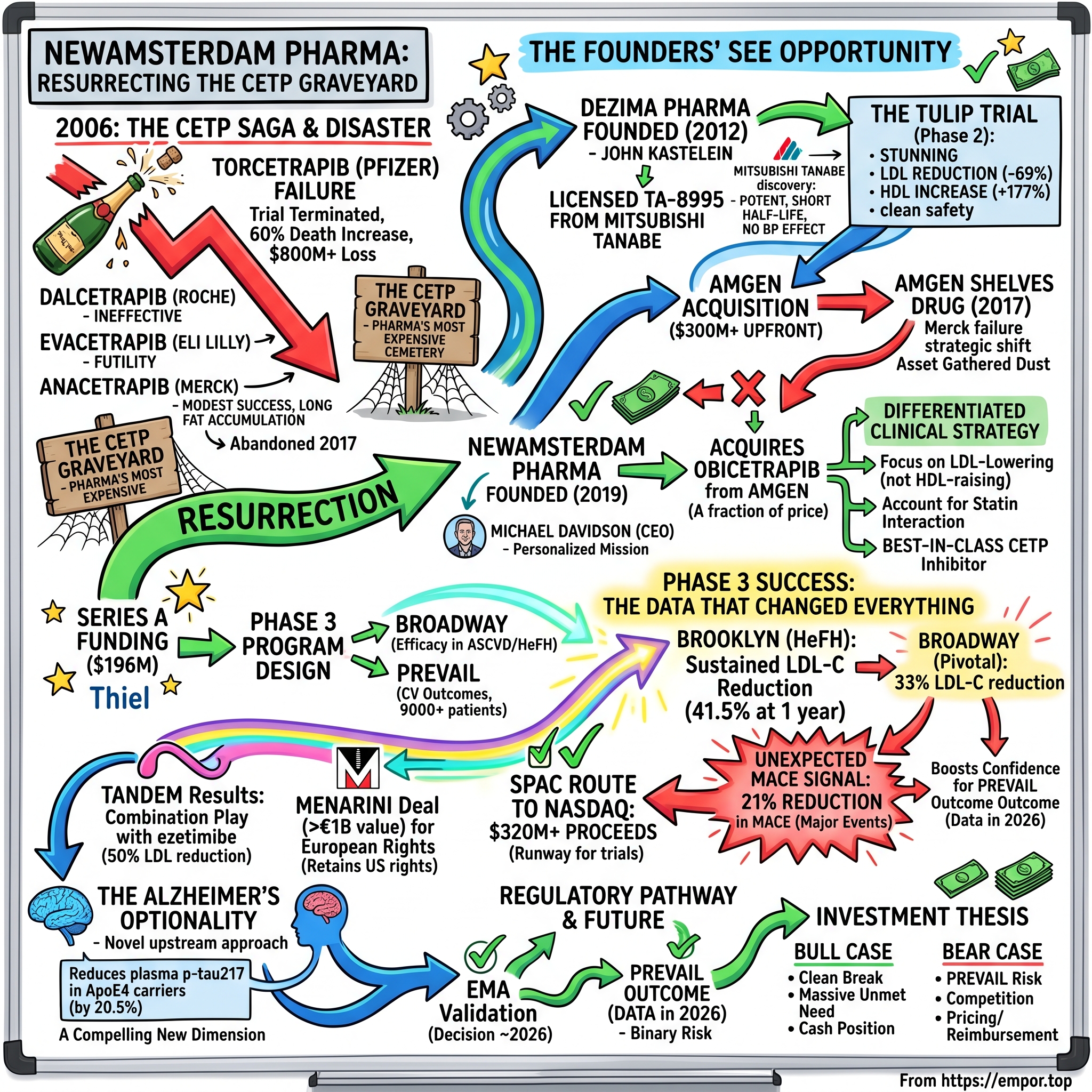
The year was 2006. Inside Pfizer's Manhattan headquarters, champagne bottles sat ready on ice. Torcetrapib, the company's most promising cardiovascular drug, was about to revolutionize heart disease treatment. Jeff Kindler, Pfizer's chief executive, proclaimed it "one of the most important compounds of our generation." Wall Street analysts projected blockbuster sales exceeding $5 billion annually.
Two days later, the bottles remained unopened—but not for celebration. Pfizer abruptly terminated torcetrapib's development after an independent monitoring committee discovered something terrifying: patients taking the drug were dying at significantly higher rates than those on placebo. On December 2, 2006, Pfizer cut off torcetrapib's phase III trial because of "an imbalance of mortality and cardiovascular events" associated with its use. In the terminated trial, a 60% increase in deaths was observed among patients taking torcetrapib and atorvastatin versus taking atorvastatin alone.
The drug cost $800 million+ to bring into Phase III development. With a single press release, Pfizer incinerated one of the largest pharmaceutical investments in history—and cast a dark shadow over an entire class of medicines called CETP inhibitors.
What followed was a decade-long trail of destruction. Anacetrapib, dalcetrapib, and evacetrapib—each representing hundreds of millions in investment—all failed. Dalcetrapib was developed by Hoffmann–La Roche until May 2012. Evacetrapib was developed by Eli Lilly and Company until October 2015. In 2017, anacetrapib's development was abandoned by Merck. The CETP graveyard had become pharma's most expensive cemetery.
Yet today, a small Dutch biotech called NewAmsterdam Pharma is attempting something that skeptics consider either visionary or delusional: resurrecting the CETP drug class with obicetrapib, a molecule originally developed in Japan, abandoned by Amgen, and now generating the kind of clinical data that has investors buzzing. The stock reached an all-time high of $41.56, reflecting a significant milestone for the biopharmaceutical company. Over the past year, the stock has experienced a remarkable increase of 94.05%, with an even more impressive 129.64% gain over the past six months.
How did the founders of this company see opportunity where the world's largest pharmaceutical giants saw only failure? The answer lies in understanding what actually killed those earlier CETP inhibitors—and why obicetrapib might be fundamentally different.
The CETP Inhibitor Saga: A Drug Class Graveyard
The Science and the Promise
To understand why Big Pharma poured billions into CETP inhibitors, you need to understand the science behind "good" and "bad" cholesterol. CETP inhibitors work by inhibiting cholesterylester transfer protein (CETP), which normally transfers cholesterol from HDL cholesterol to very low density or low density lipoproteins (VLDL or LDL). Inhibition of this process results in higher HDL cholesterol levels and reduces LDL cholesterol levels.
For decades, cardiologists believed that if low LDL cholesterol was good, then high HDL cholesterol must be even better. HDL was the "good" cholesterol that supposedly swept harmful particles out of arteries. The logic seemed bulletproof: raise HDL dramatically while lowering LDL, and you'd have a cardiovascular wonder drug that would save millions of lives.
This hypothesis attracted every major pharmaceutical company. The potential market was enormous—cardiovascular disease remains the world's leading cause of death, and statins, while effective, leave significant residual risk for many patients.
Torcetrapib: The $800 Million Disaster
Pfizer led the charge with torcetrapib, betting its future on being first to market. Pfizer developed and tested the first CETP inhibitor, torcetrapib. In the Phase 3 Investigation of Lipid Level Management to Understand Its Impact in Atherosclerotic Events (ILLUMINATE) trial, patients treated with torcetrapib had significantly higher rates of major cardiovascular and cerebrovascular events, and higher mortality resulting from cancer and infection. The trial, and all further development of torcetrapib, was terminated in December 2006.
The early data had looked spectacular. In early-phase studies in humans, the drug increased HDL cholesterol by 60 to 100% at the same time that it lowered LDL cholesterol by up to 20%. But when 15,000 patients were enrolled in the definitive outcomes trial, the results were catastrophic.
The question that haunted researchers: was this a problem with torcetrapib specifically, or with the entire CETP mechanism? It is largely accepted that off-target effects on cortisol, endothelin-1, and aldosterone led to the observed adverse outcomes. Torcetrapib raised blood pressure—a mechanism unrelated to CETP inhibition—which may have negated any cardiovascular benefits.
Dalcetrapib: Futility at Roche
Roche pushed forward with dalcetrapib, a weaker CETP inhibitor that avoided torcetrapib's blood pressure problems. The strategy was essentially "gentle CETP inhibition." Dalcetrapib, developed by Hoffman-La Roche, followed torcetrapib. In the Phase 3, Dalcetrapib in Stable Coronary Heart Disease Patients with Recent Acute Coronary Syndrome (dal-OUTCOMES) trial, treatment with dalcetrapib did not alter the risk of major cardiovascular events. The study was stopped early based on a futility analysis and Roche discontinued development of dalcetrapib in May 2012.
The drug was safe but ineffective. Since dalcetrapib is a weaker inhibitor, no effect was expected on LDL and Lp(a). It appeared that beneficial effects by HDL were offset by some detrimental factors in dalcetrapib. Being gentle had traded one problem for another: safety without efficacy.
Evacetrapib: Eli Lilly's Hope Extinguished
Eli Lilly took a different approach with evacetrapib—potent CETP inhibition without torcetrapib's off-target effects. The drug worked exactly as designed, raising HDL dramatically and lowering LDL. Surely, this would prove the hypothesis.
It didn't. The failure of the potent and seemingly "clean" evacetrapib was a major blow to the entire therapeutic hypothesis, suggesting that even ideal CETP inhibition might not be clinically effective. The ACCELERATE trial was terminated early in 2015 for futility.
This failure was particularly devastating because it suggested the problem wasn't drug-specific toxicity or insufficient potency—it might be that CETP inhibition itself simply didn't work.
Anacetrapib: Merck's Modest Success and Strategic Abandonment
Against all odds, Merck continued its REVEAL trial of anacetrapib. This history placed immense pressure on the REVEAL trial, framing it not merely as a test of Anacetrapib, but as the final, definitive referendum on the viability of the entire CETP inhibitor class. When Merck announced that REVEAL would continue after the evacetrapib failure, it was a significant strategic decision, betting that their trial's larger size and longer duration would succeed where others had failed.
The gamble partially paid off. In the study of 30,449 patients with atherosclerotic vascular disease receiving LDL-C lowering treatment with atorvastatin, anacetrapib significantly reduced the risk of major coronary events (composite of coronary death, myocardial infarction or coronary revascularization) by 9 percent relative to placebo.
A nine percent reduction was statistically significant—the first positive cardiovascular outcomes trial for any CETP inhibitor. Victory at last?
Not quite. On October 11, 2017, Merck & Co. announced that, following a thorough review of the complete clinical profile and discussions with external experts, the company would not be submitting applications for regulatory approval to the FDA or other global health authorities. Dr. Roger M. Perlmutter, then-president of Merck Research Laboratories, concluded that "the clinical profile for anacetrapib does not support regulatory filings".
Why abandon a drug that actually worked? The therapeutic benefit was attributed not to its primary HDL-raising mechanism but to a secondary reduction in non-HDL cholesterol. This, combined with its unique and concerning pharmacokinetic property of long-term accumulation in adipose tissue, created a challenging risk-benefit and commercial proposition.
Anacetrapib's fat accumulation property was unprecedented and worrying—the drug lingered in body fat for years after discontinuation. No regulator would approve it, and no patient would want to take it.
By late 2017, the CETP inhibitor class appeared definitively dead. Four drugs, four failures, billions of dollars evaporated. Every major pharmaceutical company had abandoned the field. The scientific consensus was clear: CETP inhibition was a beautiful hypothesis murdered by ugly facts.
But in the Netherlands, a small group of researchers looked at this wreckage and saw something everyone else had missed.
The Origins of Obicetrapib: Dezima Pharma & The Japanese Connection
Mitsubishi Tanabe's Discovery
Across the Pacific, Mitsubishi Tanabe Pharma Corporation had been quietly developing its own CETP inhibitor, designated TA-8995. Japanese researchers had designed a molecule with distinctive properties—highly potent, but without the structural features that had caused problems in earlier compounds. It had no apparent effect on blood pressure, no fat accumulation, and a relatively short half-life.
The molecule sat in Mitsubishi Tanabe's pipeline as a potential out-licensing candidate—interesting, but not a strategic priority for the Japanese firm.
John Kastelein: The Scientific Founder
Enter John Kastelein, a professor of medicine at the Academic Medical Center of the University of Amsterdam and one of the world's foremost lipidologists. Kastelein had spent his career studying cholesterol metabolism and had been an investigator on several of the failed CETP trials. He knew the science intimately—both its promise and its pitfalls.
Kastelein saw something in the TA-8995 data that others had overlooked. The molecule wasn't just safe—it was potently effective at lowering LDL cholesterol, not just raising HDL. The original CETP hypothesis had fixated on HDL-raising, but emerging research suggested that LDL-lowering might be the actual mechanism of cardiovascular benefit.
Dezima Pharma was founded in 2012 by John Kastelein, professor of medicine at the Department of Vascular Medicine at the Academic Medical Center of the University of Amsterdam, The Netherlands, and financed by Forbion Capital Partners, BioGeneration Ventures and New Science Ventures, and a EUR 5m loan (Innovation Credit) from the Dutch government through RVO.
The TULIP Trial: Proof of Concept
Kastelein licensed TA-8995 from Mitsubishi Tanabe and renamed it DEZ-001. The company's lead product DEZ-001 (previously TA-8995) has been in-licenced from Mitsubishi Tanabe Pharma Corporation and is a potentially best-in-class CETP inhibitor.
The Phase 2 TULIP trial results, published in The Lancet in 2015, were stunning. Data from its Phase 2 Cholesterol ester transfer protein inhibition by TA-8995 in Patients with Mild Dyslipidaemia (TULIP) trial identified several potentially advantageous properties. First, it decreased LDL-C up to 69 percent, increased HDL-C up to 177 percent, decreased apolipoprotein B (apo B) up to 51 percent, and decreased Lp(a) up to 35 percent, making it the most potent CETP inhibitor.
These numbers were remarkable—particularly the LDL reduction. Previous CETP inhibitors had shown modest LDL lowering; TA-8995 was achieving reductions comparable to PCSK9 inhibitors, the injectable biologics that were then transforming cardiovascular medicine.
Amgen's $300M Acquisition
Big Pharma noticed. Under the terms of the agreement, Amgen will pay $300 million in cash at closing and up to $1.25 billion in additional payments if certain development and sales milestones are achieved.
The September 2015 deal was audacious. The big biotech turned heads in 2015 by paying $300 million upfront to land a drug in the already tarnished CETP class. Back then, Pfizer and Roche's blow up had already dampened expectations for CETP inhibitors.
Amgen's CEO Robert Bradway explained the strategic logic: combining an oral CETP inhibitor with Amgen's newly approved injectable PCSK9 inhibitor Repatha would give the company a comprehensive cardiovascular portfolio. "With the recent launches of Repatha (evolocumab) and Corlanor (ivabradine), and today's acquisition of Dezima, Amgen is proud to be on the leading edge of an exciting new wave of treatments for cardiovascular disease."
For Kastelein and the Dezima team, it was vindication—and a substantial payday. But within two years, everything would change.
Amgen Shelves the Drug
The Merck anacetrapib decision in October 2017 sent shockwaves through the industry. In 2017, Amgen decided to discontinue the internal development of obicetrapib for strategic reasons and pursue out-licensing opportunities. Forbion believes that this drug could address very substantial unmet medical needs and therefore initiated conversations with Amgen to continue developing the asset.
Amgen has scrapped development of the CETP inhibitor it acquired in its $1.55 billion takeover of Dezima. The move sees AMG 899 join CETP inhibitors from Eli Lilly, Merck and Pfizer on the scrap heap and marks the end of leading companies' involvement with the once-hyped drug class.
Obicetrapib—now designated AMG 899—joined the graveyard. Amgen began shopping for out-licensing partners, but in a field where every major player had been burned, there were no takers.
The drug sat dormant, a $300 million asset gathering dust on Amgen's shelf.
NewAmsterdam Pharma: The Resurrection
The Return of the Founders
John Kastelein never stopped believing in obicetrapib. From his perch at the University of Amsterdam, he continued analyzing the CETP data, convinced that the scientific community had drawn the wrong conclusions. The problem wasn't CETP inhibition—it was how the trials had been designed and which patients had been enrolled.
By 2019, Kastelein and his longtime collaborators at Forbion Capital Partners decided to make an audacious bet. Founded in 2019 by the venture capital firm Forbion and John Kastelein, NewAmsterdam Pharma is a privately held, clinical-stage company focused on the research and development of transformative therapies for cardiometabolic diseases.
The company name—NewAmsterdam—evoked both the Dutch heritage of its founders and the spirit of renewal that would define its mission. They weren't just developing a drug; they were attempting to resurrect an entire therapeutic class.
Michael Davidson: A CEO With Personal Stakes
To lead the company, Kastelein recruited Michael Davidson, a cardiologist and lipidologist who had built multiple successful biotech companies. Dr. Michael Davidson, inspired by the early loss of his father to heart disease, became a cardiologist and later a life-sciences entrepreneur. When Dr. Michael Davidson was a teenager, his father died of a heart attack at the young age of 47. That early loss informed everything that followed: He decided at that moment to become a cardiologist and devote his life to helping others avoid his father's fate.
Davidson's credentials were impeccable. Board-certified in Internal Medicine, Cardiology, and Clinical Lipidology, Dr. Davidson serves as Director of the Lipid Clinic at the University of Chicago Pritzker School of Medicine and is consistently named among "Best Doctors in America." A biotech innovator, he co-founded Omthera Pharmaceuticals (acquired by AstraZeneca) and Corvidia Therapeutics (acquired by Novo Nordisk), and is the Co-founding CEO of NewAmsterdam Pharma.
Davidson brought not just scientific expertise but commercial acumen—he understood how to navigate FDA processes and build pharmaceutical companies.
The Acquisition from Amgen
In April 2020, NewAmsterdam acquired Dezima Pharma from Amgen, including all rights for obicetrapib (formerly AMG 899, now TA-8995) a selective cholesteryl ester transfer protein (CETP) inhibitor.
Financial terms were not disclosed, but industry observers estimated the price was a fraction of what Amgen had originally paid. To this end, the Company has received seed funding of approximately EUR 20M from Dutch investment firm Forbion as well as its Founders and will be raising a substantial financing round before year-end.
For Forbion, it was a full-circle moment. Sander Slootweg, Managing Partner at Forbion commented: "NewAmsterdam Pharma constitutes a very attractive investment opportunity, as obicetrapib has the potential to address the huge and poorly served patient segment of patients at risk of cardiovascular disease, currently not well controlled on statins or those even completely statin-intolerant. With over 30 million patients meeting these criteria, we believe that obicetrapib has mega-blockbuster sales potential."
The Differentiated Clinical Strategy
What made NewAmsterdam's approach different from the failures that came before? Kastelein and Davidson had developed a thesis based on careful analysis of the previous trials.
John Kastelein, CSO of NewAmsterdam Pharma concluded: "In my opinion, obicetrapib is a best-in-class CETP inhibitor. From the Phase 2b trial in nearly 400 patients, we observed an average LDL-C lowering of 45% at a 5 mg daily dose, with a clean safety profile and excellent tolerability. A key lesson from previous Phase 3 studies with other CETPi molecules is not to combine CETPi with high-dose statins, because of an observed interaction."
This insight was crucial. Previous CETP trials had enrolled patients already on high-intensity statins, potentially creating pharmacological interference that masked benefits. NewAmsterdam would design trials that accounted for this interaction.
The company also shifted focus from HDL-raising to LDL-lowering—the mechanism that actually predicted cardiovascular benefit in the anacetrapib trial.
Series A and Phase 3 Program Design
The $196M Series A
NewAmsterdam Pharma (NAP), a clinical stage company focused on the research and development of transformative therapies for cardio-metabolic diseases, today announced completion of a $196M (€160M) Series A funding round. The financing will support the full Phase 3 development of its ApoB and LDL-c lowering small molecule drug, obicetrapib.
The investor syndicate read like a who's who of life sciences venture capital. Forbion, NAP's founding investor, was joined by Morningside Ventures and Ascendant BioCapital as co-lead investors in the Series A financing. Also participating in this funding round were Kaiser Foundation Hospitals, BVF Partners L.P., Population Health Partners, LSP Dementia Fund, Peter Thiel, Janus Henderson Investors, Medpace, GL Capital, JVC Investment Partners, and Presight Capital.
Peter Thiel's participation was particularly notable—the contrarian investor known for backing transformative technologies had identified obicetrapib as exactly the kind of overlooked opportunity he seeks.
Phase 3 Trial Design
NewAmsterdam designed an ambitious Phase 3 program with multiple concurrent trials. Dosed first patients in Phase 3 BROADWAY trial and Phase 3 PREVAIL trial.
The BROADWAY trial would establish efficacy in patients with established cardiovascular disease or familial hypercholesterolemia—a challenging population that desperately needed new options.
More boldly, NewAmsterdam simultaneously launched PREVAIL, a cardiovascular outcomes trial. PREVAIL is a placebo-controlled, double-blind, randomized study in participants with a history of atherosclerotic cardiovascular disease (ASCVD) who do not have adequate control of their low-density lipoprotein cholesterol (LDL-c) despite being on maximally tolerated lipid-modifying therapies.
Starting a massive outcomes trial before completing registration trials was risky but strategic—if PREVAIL succeeded, it would provide definitive proof that CETP inhibition works, transforming obicetrapib from an LDL-lowering therapy into a drug that prevents heart attacks and strokes.
ROSE Phase 2 Results
Before Phase 3 data arrived, the company presented Phase 2 results that exceeded expectations. Over the course of 8 weeks, treatment with 5 mg or 10 mg obicetrapib resulted in a significant decrease as compared with placebo in median LDL-C concentration (by up to 51%; P < 0.0001), the primary trial outcome.
The 51% LDL reduction was remarkable—comparable to PCSK9 inhibitors but achieved with a simple oral pill. These results provided confidence for the Phase 3 program and attracted additional investors.
Menarini Deal and the SPAC Route to Nasdaq
The Menarini Licensing Agreement
In June 2022, NewAmsterdam secured a transformative partnership. Total deal value of over €1 billion; including €142.5 million upfront payment and committed R&D funding plus potential milestones and double-digit royalties on net product sales in Europe.
"Obicetrapib, if approved, could radically alter the treatment landscape in cardiovascular disease by providing an effective and oral option for hyperlipidemia patients in Europe" said Elcin Barker Ergun, Chief Executive Officer of the Menarini Group. "As a leading company in cardiovascular treatments area, we find it an excellent fit to our portfolio and look forward to collaborating with NewAmsterdam Pharma to advance its development."
The deal structure was elegant. Pursuant to the terms of the agreement, NewAmsterdam will be responsible for further clinical development of obicetrapib and the parties will cooperate in regulatory activities to secure approval for the product. Menarini will be responsible for all commercialization activities in the licensed territory.
NewAmsterdam retained U.S. rights—the world's largest pharmaceutical market—while gaining a committed European partner with deep cardiovascular expertise. The €115 million upfront payment funded ongoing trials while validating the asset's commercial potential.
The SPAC Transaction
With trials progressing and a major partnership secured, NewAmsterdam needed public market capital. In the challenging IPO environment of 2022, the company chose an unconventional route. Business combination transaction with Frazier Lifesciences Acquisition Corporation, a special purpose acquisition company sponsored by an affiliate of Frazier Healthcare Partners, completed on November 22, 2022. Closed concurrent, oversubscribed and upsized approximately $235 million private investment in public equity ("PIPE"), led by Frazier Healthcare Partners and Bain Capital Life Sciences.
The SPAC structure allowed NewAmsterdam to access public markets while avoiding the valuation compression affecting traditional biotech IPOs. The SPAC disclosed that holders of approximately 32% of FLAC Class A ordinary shares exercised their right to redeem their shares for cash, significantly lower than the average redemption rate for completed deals this year at 83.99%.
The low redemption rate—in an era when most SPACs saw 80%+ redemptions—signaled investor confidence in the NewAmsterdam story.
The ordinary shares and warrants of NewAmsterdam are expected to commence trading on the Nasdaq Capital Market under the ticker symbols "NAMS" and "NAMSW," respectively, on November 23, 2022.
The combined proceeds exceeded $320 million, providing runway through all Phase 3 readouts and beyond.
Phase 3 Success: The Data That Changed Everything
BROOKLYN Results
The first Phase 3 readout came in July 2024 with BROOKLYN, testing obicetrapib in patients with heterozygous familial hypercholesterolemia—a genetic condition causing dangerously high LDL levels. Use of obicetrapib was associated with statistically significant reductions in LDL-C when added to maximally tolerated lipid modifying therapies in patients with heterozygous familial hypercholesterolemia (HeFH), according to topline results of the phase 3 BROOKLYN trial. Announced by NewAmsterdam Pharma on July 29, 2024, topline data from the trial suggested use of the was associated with a statistically significant least squares (LS) mean reduction in LDL-C of 36.3% relative to placebo therapy at day 84 and this effect was sustained out to 1 year, with data pointing to a LS mean LDL-reduction of 41.5% at this time point.
The drug worked. In a population with limited options and critically high cardiovascular risk, obicetrapib delivered clinically meaningful LDL reduction on top of existing therapies.
BROADWAY Results: The Pivotal Moment
The real test came in December 2024 with BROADWAY, the company's largest trial. BROADWAY, the most large-scale of the three studies, comprised 2530 adults with established atherosclerotic cardiovascular disease (ASCVD) and/or HeFH, whose LDL-C was not adequately controlled despite being on maximally tolerated lipid-lowering therapy. The trial ultimately met its primary end point, as the obicetrapib 10 mg group had a least-square (LS) mean LDL-C reduction of 33% (P <.0001) compared with placebo at day 84.
But the real story wasn't the primary endpoint—it was an exploratory finding that sent the stock soaring.
The Unexpected MACE Signal
In addition, a 21% reduction in MACE favoring obicetrapib was observed. As part of the safety analysis, the trial adjudicated MACE, including death, non-fatal myocardial infarction, non-fatal stroke and coronary revascularization.
This finding was explosive. While not statistically definitive—the trial wasn't powered to prove cardiovascular outcomes—a 21% reduction in heart attacks, strokes, and cardiac deaths suggested obicetrapib might actually prevent cardiovascular events, not just lower cholesterol.
After one year, the biotech saw a 21% drop in major adverse cardiovascular events (MACE) in people on obicetrapib in an exploratory analysis. William Blair analysts said in a note to investors that the result "meaningfully exceeds our expectations."
The finding was "strong and unexpected," analysts noted, boosting confidence that the ongoing PREVAIL cardiovascular outcomes trial would succeed.
TANDEM Results: The Combination Play
NewAmsterdam's fixed-dose combination of obicetrapib with ezetimibe delivered even more impressive results. Across these studies, investigators reported low-density lipoprotein cholesterol (LDL-C) lowering of 35% to 40% with obicetrapib vs placebo as a monotherapy and LDL-C lowering of 50% vs placebo when used in combination with ezetimibe.
A 50% LDL reduction with a single daily pill—that's PCSK9 inhibitor-level efficacy without injections.
Safety Profile
Perhaps most importantly for a drug class haunted by safety failures, obicetrapib demonstrated a clean profile. Adverse events and discontinuations due to side effects were similar to placebo, consistent with what was observed in Phase 2 studies. In the safety population, there was also no increase in blood pressure, nor any difference from placebo in liver enzymes, hs-CRP, or renal function.
The absence of blood pressure effects was crucial—this was the off-target toxicity that had killed torcetrapib. Obicetrapib showed none of it.
The Alzheimer's Optionality: A Surprising Bonus
The AD Biomarker Analysis
In a development that caught even the company's management by surprise, obicetrapib showed potential benefits against Alzheimer's disease. Pre-specified analysis shows obicetrapib significantly reduced absolute levels of plasma p-tau217, a key biomarker of Alzheimer's disease pathology, in both the full analysis set (p=0.0019) and in ApoE4 carriers (p=0.0215), supporting CETP inhibition as a potential novel, upstream approach to Alzheimer's prevention.
The data, presented at the Alzheimer's Association International Conference in July 2025, showed particularly striking results in high-risk patients. In APOE4/E4 carriers, the highest risk category for Alzheimer's disease, obicetrapib reduced p-tau217 levels by 20.5%, over 12 months, compared to placebo (p=0.010).
"Today's findings mark an important early step in linking lipid biology and cardiometabolic medicine to neurodegeneration," said John Kastelein, M.D., Ph.D., FESC, Chief Scientific Officer of NewAmsterdam Pharma. "Obicetrapib's ability to reduce not only p-tau217 in ApoE4 carriers, a well-characterized and defined group, but also multiple additional important AD biomarkers would add a compelling new dimension to its therapeutic profile."
The mechanism makes biological sense. ApoE4—the genetic variant that dramatically increases Alzheimer's risk—is intimately connected to cholesterol metabolism. By modifying how cholesterol moves through the body, CETP inhibition might affect brain health as well as heart health.
Approximately two thirds of patients with Alzheimer's disease carry the ApoE4 risk isoform that is associated with a much greater risk of developing AD.
If these findings translate to clinical benefit, obicetrapib could become one of the first drugs to simultaneously address both cardiovascular and neurodegenerative disease—a massive expansion of its addressable market.
Regulatory Pathway and Market Opportunity
European Filing
NewAmsterdam's partnership with Menarini has accelerated European regulatory progress. The European Medicines Agency (EMA) has validated NewAmsterdam Pharma's marketing authorization application (MAA) for investigational obicetrapib and its fixed-dose combination with ezetimibe as potential treatments for patients with hypercholesterolemia, including both heterozygous familial (HeFH) and non-familial or mixed dyslipidemia.
The EMA validation represents a significant milestone, with a decision potentially coming in 2026.
The PREVAIL Outcome
The company's most important catalyst remains the PREVAIL cardiovascular outcomes trial. The Company also commenced the Phase 3 PREVAIL cardiovascular outcomes trial in March 2022, which is designed to assess the potential of obicetrapib to reduce occurrences of major adverse cardiovascular events, including cardiovascular death, non-fatal myocardial infarction, non-fatal stroke and non-elective coronary revascularization.
NewAmsterdam Pharma Company N.V. today announced that it has met the enrollment target of 9,000 patients for the pivotal Phase 3 PREVAIL cardiovascular outcomes trial evaluating obicetrapib in adult patients with a history of atherosclerotic cardiovascular disease. Driven by strong patient and physician interest globally, NewAmsterdam will extend enrollment to the end of April where we expect to randomize over 9,000 patients.
Data are expected in 2026, and the exploratory MACE signal from BROADWAY suggests the trial has a real chance of success.
The Investment Thesis: Bull vs. Bear
The Bull Case
1. Clean Break from CETP Failures
Obicetrapib has demonstrated excellent safety and tolerability in more than 600 patients in phase 1 and 2 clinical trials and several thousand patients enrolled in the phase 3 program to date. There have been no clinically relevant changes in vital signs, 12-lead electrocardiograms, hematology, biochemistry, or physical examinations.
Unlike torcetrapib's blood pressure problems, dalcetrapib's weak efficacy, and anacetrapib's fat accumulation, obicetrapib appears to be the "Goldilocks" CETP inhibitor—potent enough to work, safe enough to take.
2. Massive Unmet Need
More than 100 million people globally are not achieving LDL-c goals despite the current available standard of care.
With statins generic and PCSK9 inhibitors requiring injections, an oral drug that delivers comparable LDL reduction would address a huge treatment gap.
3. Multiple Value Drivers
The cardiovascular indication alone justifies the current valuation, but the Alzheimer's data adds significant optionality. Additionally, the company retains U.S. commercial rights, preserving the upside from the world's largest pharmaceutical market.
4. Strong Cash Position
As of June 30, 2025, NewAmsterdam recorded cash, cash equivalents and marketable securities of $783.3 million.
This runway extends well past all key catalysts, reducing financing risk.
The Bear Case
1. PREVAIL Binary Risk
The entire thesis hinges on proving cardiovascular outcomes. If PREVAIL fails—if obicetrapib lowers LDL but doesn't reduce heart attacks—the drug's commercial potential collapses dramatically. The MACE signal from BROADWAY is encouraging but not definitive.
2. Competition
The lipid-lowering landscape is evolving rapidly. Oral PCSK9 inhibitors are advancing in development, and drugs targeting lipoprotein(a) could change how physicians approach residual cardiovascular risk. Even if obicetrapib succeeds, it may face intense competition.
3. Pricing and Reimbursement Uncertainty
In an era of drug price scrutiny, an expensive new cholesterol medication may face reimbursement challenges. The value proposition depends on outcomes data that won't be available until 2026.
4. CETP Skepticism Persists
After $15+ billion in failed CETP investments by Big Pharma, some physicians and payers may remain skeptical regardless of the data. Changing deeply ingrained perceptions requires time and resources.
Porter's Five Forces Analysis
| Force | Assessment | Implications |
|---|---|---|
| Threat of New Entrants | Moderate | High clinical and regulatory barriers, but multiple companies pursuing novel lipid-lowering approaches |
| Bargaining Power of Buyers | High | Large payers (PBMs, government) have significant leverage over cardiovascular drug pricing |
| Bargaining Power of Suppliers | Low | API manufacturing well-established; no proprietary raw materials |
| Threat of Substitutes | High | Generic statins, injectable PCSK9 inhibitors, ezetimibe all compete for the same patients |
| Competitive Rivalry | Moderate | Few oral alternatives with this efficacy, but significant pipeline competition |
Hamilton Helmer's 7 Powers Framework
Potential Power Sources:
-
Counter-Positioning: NewAmsterdam has taken a contrarian position against industry consensus that CETP inhibition doesn't work. If PREVAIL succeeds, this contrarian bet delivers extraordinary returns precisely because incumbents abandoned the space.
-
Cornered Resource: The obicetrapib molecule itself is a scarce asset—the only remaining high-quality CETP inhibitor in development—giving NewAmsterdam exclusive access to a potentially validated mechanism.
-
Process Power: The team's deep experience from previous CETP failures has informed superior trial design, potentially enabling success where others failed.
Power Not Yet Established:
- Scale Economies, Network Effects, Switching Costs, and Branding remain largely theoretical until commercial launch and PREVAIL data.
Key Performance Indicators for Investors
For long-term investors tracking NewAmsterdam Pharma, two metrics stand above all others:
1. PREVAIL Trial Event Rate and Hazard Ratio The cardiovascular outcomes trial represents the make-or-break moment for the company. Investors should track: - Target event accumulation toward statistical significance - Any interim analysis announcements - Hazard ratio magnitude when data are released (likely 2026)
A statistically significant reduction in MACE—ideally 15-20%+ relative risk reduction—would validate the CETP mechanism and transform obicetrapib's commercial potential. Failure here would severely impair the thesis.
2. Regulatory Timeline Adherence With the EMA MAA now validated and U.S. filing discussions underway: - Monitor milestone payments from Menarini (indicating partnership health) - Track FDA interaction outcomes (breakthrough therapy designation requests, etc.) - Watch for approval timelines in Europe and the U.S.
Delays in regulatory progress or unexpected FDA requests for additional data would signal execution risk.
Conclusion: The Ultimate Drug Resurrection Story
NewAmsterdam Pharma's story encapsulates everything fascinating about pharmaceutical development: the audacity of scientific conviction, the patience required for multi-year clinical trials, and the enormous financial stakes involved in bringing new medicines to market.
If ultimately approved, obicetrapib would be the first CETP inhibitor to reach market and change the narrative surrounding the drugs, which were largely abandoned by pharmaceutical companies last decade due to poor clinical performance and safety concerns. Yet, obicetrapib would compete with an array of other therapies, among them generic statins and injectable PCSK9 inhibitors.
The company represents a rare species: a second chance at a discarded asset, executed by founders who understood the original failure better than anyone. John Kastelein didn't just believe in CETP inhibition—he had intimate knowledge of exactly why previous drugs failed and how obicetrapib might be different.
The Phase 3 data vindicate the scientific thesis: obicetrapib potently lowers LDL cholesterol with a safety profile comparable to placebo. The exploratory MACE signal from BROADWAY suggests the mechanism may indeed prevent cardiovascular events—exactly what the original CETP hypothesis promised but previous drugs never delivered.
The Alzheimer's optionality adds another layer. In a world desperate for Alzheimer's prevention therapies, a drug that might slow neurodegeneration while protecting the heart would be transformative.
But substantial risks remain. PREVAIL is a large, complex outcomes trial, and cardiovascular outcomes trials have humbled many companies before. The 21% MACE signal is encouraging but not definitive. Competition is intensifying across the lipid-lowering space.
What makes NewAmsterdam's story compelling is the rare combination of scientific rigor, experienced leadership, and financial firepower. The company isn't betting on hope—it's betting on a differentiated molecule, deep understanding of previous failures, and carefully designed trials that address historical weaknesses.
Whether obicetrapib ultimately succeeds or fails, NewAmsterdam Pharma has already achieved something remarkable: forcing the scientific community to reconsider a drug class everyone else had written off. In the graveyard of CETP inhibitors, one molecule has risen—and the next 18 months will determine whether that resurrection becomes permanent.
 RSS Feed
RSS Feed Spotify
Spotify Apple Podcasts
Apple Podcasts Amazon Music
Amazon Music Audible
Audible YouTube
YouTube