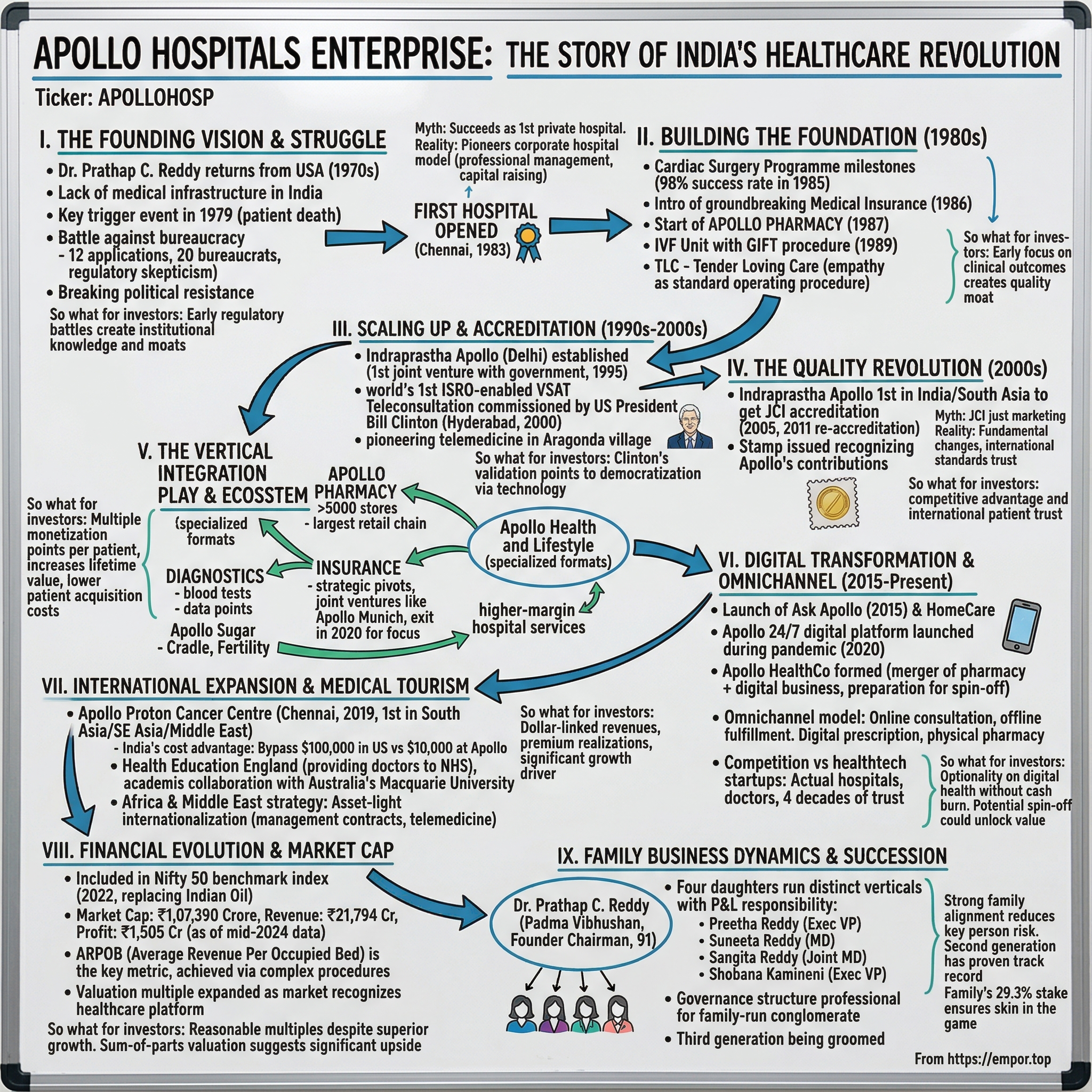
Apollo Hospitals Enterprise: The Story of India's Healthcare Revolution
I. Introduction & Episode Setup
Picture this scene: September 1983, Chennai. A cardiologist who'd spent years treating American patients in Missouri stands in the gleaming corridors of India's first corporate hospital. The skeptics called him a fool. The government bureaucrats made him wait in their offices for months. The banks refused to lend money for what they saw as a "luxury" venture. Yet here was Dr. Prathap C. Reddy, watching President Zail Singh cut the ribbon on what would become Asia's healthcare giant.
The first Apollo hospital in Chennai was inaugurated by Zail Singh, then President of India, in 1983. This wasn't just another hospital opening—it was the birth of India's private healthcare revolution.
Today, Apollo Hospitals Enterprise is the largest for-profit private hospital network in India, with a network of 71 owned and managed hospitals. The company commands a market capitalisation of Rs 1,07,390 crore, making it one of India's most valuable healthcare enterprises. But the real paradox isn't the size—it's the origin story. How does a doctor who could have lived comfortably treating wealthy Americans in Boston end up battling Indian bureaucracy to build hospitals? And why would anyone leave the world's most advanced healthcare system to return to a country where patients routinely flew abroad for basic surgeries?
This is a story about more than hospitals. It's about vertical integration mastery—from pharmacies to insurance to digital health. It's about family business dynamics where four daughters each play crucial roles: Preetha Reddy, the eldest, is Executive Vice Chairperson; Shobana Kamineni, the third daughter, is also Executive Vice Chairperson; Suneeta Reddy, the second, is Managing Director; and the youngest, Sangita Reddy, is Joint Managing Director. And it's about transforming an entire nation's approach to healthcare, one patient at a time.
So what for investors: Apollo represents a unique play on India's healthcare transformation—a founder-led business with proven execution across multiple healthcare verticals, now trading at compelling valuations relative to its growth trajectory.
II. The Founding Story & Dr. Prathap Reddy's Vision
The letter arrived on a humid Boston evening in 1970. Dr. Reddy had received his medical degree from Stanley Medical College in Chennai and later trained as a Cardiologist in the UK and USA. He did his Fellowship from the Massachusetts General Hospital, Boston and went on to head several research programs at the Missouri State Chest Hospital, USA. His practice was thriving, his reputation growing. But the letter from his father changed everything. In those days, an Indian father's request to return home wasn't a suggestion—it was a summons.
Reddy and his family decided to return to India in the early 1970s. Back in Chennai, his practice flourished, but he also faced a stark reality: a lack of medical infrastructure. He was forced to refer most of his patients who needed complex surgeries to friends in the US. Many were referred to pioneering heart surgeon, Dr Denton Cooley.
The trigger moment came in 1979. Reddy referred a patient to the US. But the man's family could not raise the money required. And despite Reddy's best efforts, he did not survive. This wasn't just a medical failure—it was a systemic one. Here was a patient who could have been saved with the right infrastructure, dying because India lacked what America took for granted: corporate hospitals with modern equipment and protocols.
But building a corporate hospital in 1980s India was like trying to sell ice to Eskimos—nobody understood why you'd need it. Till Dr Reddy came up with his project, one was not allowed to go to the market to raise funds or go to banks and financial institutions to borrow to set up hospitals. The profit motive was a strict no no. There were government hospitals and hospitals set up by trusts. Mindsets were rigid and there was enormous resistance to healthcare as a business.
"The moment they heard that I was wanting to do this, people called me a fool. So that became my strength," Dr Reddy revealed. The regulatory battles were Kafkaesque. He had to make many pilgrimages to see Dr. Manmohan Singh, then the governor of RBI, and the then finance minister Pranab Mukerjee. He had to make 12 applications to 20 babus. He had to spend 2 days every week in Delhi. All this was to get permission to make the initial public offering.
The breakthrough came through an unlikely ally. On one such trip, he managed to meet then Prime Minister Indira Gandhi. Finally, with the government's support, he opened the first Apollo hospital in Chennai. But even with political backing, it took the doctor three years to get the necessary permissions.
The name itself carried ambition. Suneeta, his second daughter, clarified that it was inspired by the Greek god Apollo, known for his healing abilities. "I decided on 'Apollo Hospitals' to convey a global message, signifying India's prowess in healthcare. My vision extended beyond a single hospital, aiming to establish many".
Myth vs Reality Box: Myth: Apollo succeeded because it was India's first private hospital. Reality: Private nursing homes existed before Apollo. What Apollo pioneered was the corporate hospital model—professional management, ability to raise capital from markets, and standardized protocols across facilities.
So what for investors: Regulatory moats matter. Apollo's early struggles with bureaucracy created institutional knowledge that competitors still struggle to replicate, particularly in navigating India's complex healthcare regulations.
III. Building the Foundation: The 1980s Expansion
The numbers from Apollo's first years read like fiction. By 1985, the Cardiac Surgery Programme hit a big milestone. They completed 100 surgeries with a 98% success rate. Apollo quickly became a leader in cardiac care. In an era when Indian healthcare was synonymous with government hospitals and charitable trusts, here was a private company achieving world-class outcomes.
In its first year Apollo had a success rate of 97 per cent in heart operations. The next year 700 surgeries were performed and the success rate was 97.7 per cent. These weren't just statistics—they were validation of a model everyone said couldn't work.
The financial innovation came in 1986. Apollo Hospitals introduced a groundbreaking Medical Insurance scheme with United India Insurance Company Limited. Think about the audacity here: in a country where health insurance barely existed, Apollo was creating the market for its own services. This wasn't just treating patients—it was building the entire ecosystem.
By 1987, two critical developments shaped Apollo's future. First, Apollo had performed over 700 open-heart surgeries. Second, and perhaps more importantly for long-term strategy, Apollo Pharmacy was started in 1987. This wasn't just backward integration—it was the beginning of Apollo's transformation from a hospital company to a healthcare conglomerate.
The culture Dr. Reddy instilled was distinctive. At the core of Apollo's patient-centric culture is TLC (Tender Loving Care), the magic that inspires hope amongst its patients. In a country where government hospitals treated patients as numbers, Apollo introduced something revolutionary: empathy as standard operating procedure.
Then came 1989, and another breakthrough. Apollo made medical history with its IVF Unit, helping a baby enter the world through the 'GIFT' procedure. The GIFT (Gamete Intrafallopian Transfer) technique represented Apollo's ambition to bring cutting-edge medical procedures to India, not years after they were proven in the West, but contemporaneously.
By 1987, the hospital was able to show a profit. Mistakes were made and these led to good systems being developed. The critics who said corporate healthcare couldn't work in India were watching Apollo not just survive, but thrive.
The family structure that would define Apollo for decades was taking shape. While Dr. Reddy remained the visionary patriarch, his daughters weren't just inheritors—they were builders. Each found their niche: operations, finance, pharmacy, digital initiatives. This wasn't nepotism; it was strategic deployment of family members who'd grown up breathing the business.
So what for investors: Apollo's early focus on clinical outcomes over rapid expansion created a quality moat that still drives premium pricing today. The 98% success rate in cardiac surgeries became marketing that money couldn't buy.
IV. Scaling Up: International Accreditation & Specialization (1990s–2000s)
The 1990s opened with recognition. Dr. Reddy received the Padma Bhushan in 1991, but the real prize was what came next. In 1995, Indraprastha Apollo Hospital was established as the third super specialty tertiary care hospital set by the Apollo Hospitals Group, jointly with the Government of Delhi. This wasn't just another hospital—it was Apollo's first joint venture with a state government, proving the model could work beyond private capital.
The Delhi project was massive in scope. It is a 695-bed hospital, with the provision for expansion to 1000 beds in future. The hospital is spread over 15 acres, and has a built-up area of 600,000 square feet. For context, most Indian hospitals at the time operated out of converted residential buildings. Apollo was building healthcare cities.
But the real revolution came in 2000, in an unlikely place. On March 24th 2000, the world's first Teleconsultation from a village hospital through an ISRO enabled VSAT was commissioned by the then US president Bill Clinton from Hyderabad in the presence of the then Chief Minister Sri Chandrababu Naidu. The location was significant: Apollo developed telemedicine services, after starting a pilot project in 2000 at Aragonda, Prathap Reddy's home village.
Bill Clinton's presence wasn't just diplomatic courtesy. Speaking on the occasion Clinton remarked "I think it is a wonderful contribution, to the healthcare of the people living in villages". Here was the leader of the world's most powerful nation validating Apollo's vision of using technology to democratize healthcare.
The quality revolution reached its apex in 2005. Indraprastha Apollo Hospital was accredited by Joint Commission International (JCI) USA as the first internationally accredited Hospital in India in 2005 and South Asia. In 2011, the hospital got re-accredited by JCI for a fourth time consequently, making it the first hospital in India to do so.
JCI accreditation wasn't just a certificate to hang on the wall. It was validation that an Indian hospital could meet the same standards as Cleveland Clinic or Mayo. It meant international patients could trust Apollo with their lives. It meant insurance companies worldwide would recognize Apollo treatments.
The government took notice. The Government of India had issued a commemorative stamp in recognition of Apollo's widespread contributions, the first for a healthcare organization. In addition, a stamp was also released to mark the 15th anniversary of India's 1st successful liver transplant performed at Apollo Hospitals.
Myth vs Reality Box: Myth: Apollo's JCI accreditation was just marketing. Reality: JCI required fundamental process changes—from hand hygiene protocols to medication management systems. Apollo spent millions redesigning workflows to meet international standards.
So what for investors: International accreditation created a sustainable competitive advantage. Even today, only a handful of Indian hospitals maintain JCI certification due to its cost and complexity.
V. The Vertical Integration Play: Building the Healthcare Ecosystem
Apollo's business model is deceptively simple on paper but fiendishly complex in execution. Apollo Pharmacy is the largest retail pharmacy chain in India with more than 5,000 stores in over 21 states. But this isn't just about selling medicines—it's about controlling the entire patient journey.
The acquisition strategy was aggressive. In 2014, Apollo Hospitals acquired Hetero Med Solutions, a South Indian pharmacy chain with 320 stores, from Hetero Group for ₹146 crore (US$23.92 million) in a slump sale. The stores were rebranded as Apollo Pharmacy. This wasn't empire building—it was ecosystem creation.
The diagnostics play followed similar logic. When a patient needs a blood test, where do they go? Apollo Diagnostics. When they need medicines? Apollo Pharmacy. Primary care? Apollo Clinics. Each touchpoint isn't just a revenue stream—it's a data point, a relationship builder, a funnel to higher-margin hospital services.
The insurance ventures tell a different story—one of strategic pivots. Apollo entered health insurance through joint ventures, first with DKV AG creating Apollo DKV Insurance, later rebranded as Apollo Munich. But in 2020, Apollo Hospitals sold its 50.80% percent majority stake in Apollo Munich Health Insurance to HDFC for ₹1,495 crore (US$201.76 million). The exit wasn't failure—it was focus. Apollo realized its competitive advantage lay in providing healthcare, not financing it.
Apollo Health and Lifestyle became the umbrella for specialized formats. Think of it as the "specialty retail" of healthcare—Apollo Sugar for diabetes, Apollo Cradle for maternity, Apollo Fertility for IVF, Apollo Dialysis for renal care. Each vertical targets a specific patient segment with specialized services, higher margins, and recurring revenue models.
The integration goes deeper than ownership. A patient visiting Apollo Pharmacy for diabetes medication might be referred to Apollo Sugar clinics for specialized care. If complications arise, they're seamlessly transferred to Apollo Hospitals. The electronic health records follow them throughout, creating switching costs that would make a SaaS company envious.
So what for investors: The vertical integration strategy creates multiple monetization points per patient and increases lifetime value. The pharmacy-to-hospital funnel alone drives significant patient acquisition at lower costs than traditional marketing.
VI. Digital Transformation & Apollo 24/7 (2015–Present)
October 2015 marked a pivot that few saw coming. Apollo launched home care services under Apollo HomeCare and its digital healthcare platform called Ask Apollo. This was five years before COVID made telemedicine mainstream. Apollo was building for a future that hadn't arrived yet.
The pandemic changed everything. Apollo 24/7 is the digital healthcare platform of the group which was launched in 2020. But unlike pure-play healthtech startups burning venture capital, Apollo had an unfair advantage: actual hospitals, real doctors, and four decades of trust.
Apollo HealthCo was formed in 2021 with the merger of the group's non-hospital pharmacy chain Apollo Pharmacy and its digital healthcare business known as Apollo 24/7. This wasn't just organizational restructuring—it was preparation for a potential spin-off, creating a separate digital health entity that could be valued on tech multiples rather than hospital multiples.
The competition with new-age healthtech startups is fascinating. Practo, 1mg, PharmEasy—all raised hundreds of millions to build what Apollo already had: pharmacy networks, diagnostic capabilities, doctor consultations. But they lacked what Apollo possessed: the ability to escalate care seamlessly from app to ICU.
Apollo's approach to digital is distinctly different from startups. While others focus on user acquisition at any cost, Apollo focuses on user activation—converting app downloads into actual healthcare consumption. A consultation on Apollo 24/7 can lead to diagnostics at Apollo labs, medicines from Apollo Pharmacy, and if needed, admission to Apollo Hospitals.
The omnichannel model is where Apollo's strategy crystallizes. Online consultation, offline fulfillment. Digital prescription, physical pharmacy. Virtual follow-up, in-person surgery. It's not either/or—it's both/and.
So what for investors: Apollo 24/7 represents optionality on digital health without the cash burn of pure-play startups. The potential spin-off could unlock significant value as markets value digital health platforms at premium multiples.
VII. International Expansion & Medical Tourism
In January 2019, Apollo opened Apollo Proton Cancer Centre in Chennai, which is reportedly the first proton therapy facility across South Asia, Southeast Asia and the Middle East. This wasn't just another cancer center—it was a $150 million bet that patients from Dubai to Dhaka would fly to Chennai for treatment.
The medical tourism opportunity is massive but nuanced. India's cost advantage is real—a heart bypass that costs $100,000 in the US costs $10,000 at Apollo with comparable outcomes. But cost alone doesn't drive medical tourism. Trust does. Quality does. And increasingly, technology does.
The partnerships strategy reveals Apollo's international ambitions. Apollo signed an MoU with Health Education England in April 2017 to provide a large number of doctors to fill vacancies in the English National Health Service. This wasn't labor arbitrage—it was capability signaling. If Apollo doctors are good enough for the NHS, they're good enough for anyone.
In September 2017, Apollo announced an academic collaboration with Australia's Macquarie University, where students enrolled in Macquarie's four-year graduate entry Doctor of Medicine program would complete 5 months of clinical rotations at Apollo hospitals in Hyderabad as part of their degree. Australian medical students training in Indian hospitals—a reversal of traditional flows that would have been unthinkable in 1983.
The Africa and Middle East strategy is particularly interesting. Rather than building hospitals abroad (capital intensive, regulatory complex), Apollo focuses on management contracts and telemedicine partnerships. It's asset-light internationalization—exporting expertise rather than infrastructure.
So what for investors: Medical tourism provides dollar-linked revenues and premium realizations. As more countries recognize Indian healthcare quality, this could become a significant growth driver with better margins than domestic business.
VIII. Capital Markets Journey & Financial Evolution
March 2022 marked a watershed moment. Apollo Hospitals was included in Nifty 50 benchmark index, replacing Indian Oil, and became the first hospital company to be included in the index. A hospital company replacing an oil PSU in India's premier index—the symbolism wasn't lost on anyone.
The economics of hospital operations are brutal. High capex (building hospitals), long gestation (3-5 years to break even), working capital intensive (insurance companies pay after 45-90 days), and regulated pricing in many procedures. Yet Apollo has cracked the code.
ARPOB (Average Revenue Per Occupied Bed) is the metric that matters. Apollo consistently achieves ARPOB 50-70% higher than competition through case mix optimization—more complex procedures, shorter lengths of stay, better insurance coverage. It's not about filling beds; it's about filling them with the right patients.
The capital allocation journey shows evolution. Early years: build hospitals. Middle years: acquire pharmacies. Recent years: invest in digital. The company has deployed over ₹15,000 crore in capex over four decades, creating assets that would be impossible to replicate today at any cost.
Apollo Hospitals has a market cap of 1,01,864 Crore with revenue of 21,794 Cr and profit of 1,505 Cr. The valuation multiple has expanded as markets recognize Apollo isn't just a hospital company—it's a healthcare platform.
So what for investors: Apollo trades at reasonable multiples relative to global hospital chains despite superior growth. The sum-of-parts valuation (hospitals + pharmacy + digital) suggests significant upside as businesses mature.
IX. The Family Business Dynamics & Succession
Dr. Prathap C Reddy, Founder Chairman of the Apollo Hospitals Group has been conferred with the prestigious Padma Vibhushan, India's second highest civilian award. But the real achievement isn't the awards—it's building an institution that can outlive its founder.
The four daughters aren't figureheads. Dr. Suneeta Reddy, the Managing Director of Apollo Hospitals, is renowned for her visionary leadership and relentless pursuit of excellence in the healthcare industry. With her at the helm since 1989, Apollo Hospitals has flourished as Asia's most trusted healthcare provider.
Each daughter runs a distinct vertical with P&L responsibility. There's no overlap, no confusion, no palace intrigue. The governance structure is surprisingly professional for a family-run Indian conglomerate—independent directors have real power, audit committees have teeth, and the board isn't a rubber stamp.
The comparison with other Indian family businesses is instructive. Unlike the Ambani brothers who split Reliance, or the Bajaj family feuds, Apollo has maintained unity through clear role definition. It's the Murugappa Group model—family provides vision and values; professionals execute strategy.
Succession planning is already visible. The third generation is being groomed, but not guaranteed positions. They must prove themselves, often starting in junior roles and rotating through divisions. It's meritocracy with a family safety net.
So what for investors: Strong family alignment reduces key person risk. The second generation's proven track record suggests succession won't disrupt operations. The family's 29.3% stake ensures skin in the game without blocking institutional influence.
X. Playbook: Business & Investing Lessons
Building Trust in Healthcare: Apollo's moat isn't technology or infrastructure—it's trust. In healthcare, trust takes decades to build and moments to destroy. Every successful surgery adds to the trust bank; every medical negligence case makes withdrawals. Apollo's obsessive focus on clinical outcomes over financial metrics in early years created a trust surplus that competitors still can't match.
Vertical Integration in Fragmented Markets: India's healthcare market is intensely fragmented—thousands of standalone hospitals, pharmacies, and diagnostic centers. Apollo's vertical integration strategy works because it brings order to chaos. Patients value the convenience of integrated care. Insurers value the standardized protocols. The government values the organized sector's compliance.
Network Effects in Healthcare: Every Apollo Pharmacy customer is a potential Apollo Hospital patient. Every Apollo 24/7 app user is a potential Apollo Diagnostics customer. The network effects aren't as strong as social media, but they're more defensible—switching costs in healthcare are high when your medical records, doctor relationships, and trust are invested in one ecosystem.
Capital Allocation in Asset-Heavy Businesses: Hospitals are capital black holes—one 500-bed hospital costs ₹500-1000 crore to build. Apollo's capital allocation evolved from pure hospital building to asset-light formats (clinics, pharmacies) to digital platforms. The ROCE improved from single digits to mid-teens as the mix shifted.
The Economics of Quality: Apollo's premium positioning seemed irrational in a price-sensitive market like India. But healthcare has peculiar economics—nobody wants the cheapest heart surgery. By targeting the top 20% who could afford quality, Apollo built a sustainable business model. As India's middle class expanded, Apollo's addressable market grew without lowering standards.
So what for investors: The playbook is replicable but execution is not. Several hospital chains have tried copying Apollo's model but struggle with execution complexity. The moat is in operational excellence, not strategy.
XI. Competition & Industry Analysis
The competitive landscape reads like a medical drama. Fortis Healthcare, once Apollo's biggest rival, imploded in a promoter fraud scandal. Max Healthcare, backed by private equity, focuses on North India. Manipal and Narayana target different segments—Manipal goes premium, Narayana goes mass.
The real competition isn't other hospital chains—it's the government. Ayushman Bharat, the world's largest government health insurance scheme, covers 500 million Indians for basic healthcare. It's both threat and opportunity. Threat because it sets price caps. Opportunity because it expands the insured population.
Standalone specialty chains are nibbling at the edges. Fertility chains like Nova IVI. Eye hospitals like Vasan. Dental chains like Clove. Each targets a specific vertical Apollo also operates in. But Apollo's integrated model means a patient needing multiple services stays within the ecosystem.
The international competition is intensifying. Medical tourists now have options—Thailand's Bumrungrad, Singapore's Mount Elizabeth, Dubai's American Hospital. Apollo's advantage is cost, but as Indian costs rise and competitor quality improves, the gap narrows.
The healthtech disruption is overhyped but real. Startups unbundle Apollo's services—Practo for consultations, 1mg for pharmacy, Thyrocare for diagnostics. But healthcare isn't commerce. When you're sick, you want integration, not aggregation.
Myth vs Reality Box: Myth: Digital health startups will disrupt traditional hospitals. Reality: Healthcare is inherently physical. Startups are creating new consumption occasions (preventive health, chronic management) rather than replacing hospitals.
So what for investors: Apollo faces competition on multiple fronts but has defended market share through service quality and brand strength. The integrated model becomes more valuable as healthcare becomes more complex.
XII. Bear vs. Bull Case
Bear Case:
Regulatory risks loom large. The government could cap procedure prices, mandate free treatment quotas, or change insurance reimbursements. In March 2025, the Supreme Court warned Indraprastha Apollo Hospital that it will direct AIIMS to take over if free treatment wasn't provided to poor patients in accordance with the original lease agreement. Every government hospital that partners with Apollo comes with social obligations.
Competition is intensifying on all fronts. New hospital chains backed by private equity are emerging. Digital health startups are raising massive rounds. Government hospitals are upgrading infrastructure. Apollo's premium pricing faces pressure.
The capital intensity remains brutal. Each new hospital is a ₹500-1000 crore bet with 3-5 year payback. Meanwhile, asset-light digital health companies achieve unicorn valuations without owning a single bed. Markets might rerate Apollo as a slow-growth, capital-intensive business.
Execution risks in digital transformation are real. Apollo 24/7 competes with venture-funded startups that can afford to burn cash for growth. Apollo must balance profitability with growth—a tightrope walk that many traditional companies fail.
Concentration risk in metro markets is concerning. 70% of revenues come from top 8 cities. As metro markets saturate, growth must come from Tier 2/3 cities where Apollo's premium positioning is harder to sustain.
Bull Case:
The under-penetrated healthcare market offers decades of growth. India has 0.7 hospital beds per 1,000 population versus WHO recommendation of 3.5. Healthcare spending is 3.5% of GDP versus 10%+ in developed markets. The runway is long.
Apollo Hospitals's current revenue (TTM) is ₹219.42 Billion. In 2024 the company made revenue of ₹209.48 Billion, an increase over the revenue in 2023 that were of ₹182.49 Billion. The growth momentum remains strong despite the base effect.
The integrated ecosystem creates powerful switching costs. A patient with their health records in Apollo's system, relationships with Apollo doctors, and trust in Apollo's brand won't switch for marginal cost savings. The lifetime value of customers keeps increasing.
Digital health isn't a threat—it's an opportunity. Apollo 24/7 can achieve tech valuations while leveraging Apollo's physical infrastructure. The potential spin-off could unlock significant value—pharmacy and digital businesses could be worth more than the current market cap.
Medical tourism provides a dollar hedge and premium realizations. As more international patients discover India's cost-quality equation, Apollo is best positioned to capture this demand with JCI accreditations and proton therapy capabilities.
So what for investors: The bear case risks are real but manageable. The bull case isn't about multiple expansion—it's about steady compounding in an under-penetrated market with high barriers to entry.
XIII. The Future: What's Next for Apollo
"Touch a Billion Lives"—that's Apollo's stated vision. It sounds audacious until you do the math. With 150 million patients already served and digital platforms scaling rapidly, a billion isn't impossible—it's inevitable.
AI in healthcare isn't science fiction at Apollo. They're using AI for radiology reads, predicting ICU deterioration, and optimizing bed allocation. But the real opportunity is in preventive healthcare—using data from millions of patients to predict and prevent disease.
The next generation of leadership is already visible. The founder is 91 but still works 20-hour days. The second generation has proven operational capability. The third generation brings digital nativity. The transition will be gradual, not disruptive.
International expansion will likely remain asset-light—management contracts, telemedicine partnerships, and medical education collaborations rather than building hospitals abroad. The capital is better deployed in India where returns are higher.
The strategic priorities are clear: densify existing markets rather than aggressive geographic expansion, integrate digital and physical channels seamlessly, and maintain clinical excellence while improving affordability. It's execution that matters now, not strategy.
So what for investors: Apollo's future value creation will come from operating leverage in existing assets, digital platform scaling, and medical tourism growth rather than aggressive hospital additions. The company is transitioning from growth to optimization phase.
XIV. Epilogue & Key Takeaways
The transformation of Indian healthcare is inseparable from Apollo's story. When Dr. Reddy opened that first hospital in 1983, India's healthcare was binary—government hospitals for the masses, foreign travel for the rich. Today, India performs complex procedures that attract patients from developed countries.
For entrepreneurs in regulated industries, Apollo offers crucial lessons. First, regulatory complexity is a moat, not just a barrier. Second, building trust in critical services takes time—there are no shortcuts. Third, vertical integration makes sense when the ecosystem is fragmented.
The power of purpose-driven business is evident. Apollo succeeded not despite its focus on clinical outcomes over profits, but because of it. In healthcare, doing good and doing well aren't mutually exclusive—they're mutually reinforcing.
Building lasting institutions in emerging markets requires patient capital, operational excellence, and strategic patience. Apollo spent 40 years building what can't be replicated with venture capital—trust, expertise, and integrated infrastructure.
The final reflection is personal. Dr. Reddy could have remained a successful cardiologist in America. Instead, he chose the harder path of building healthcare infrastructure in India. That choice has saved millions of lives and created billions in value. Sometimes, the best investment is betting on purpose-driven founders who see beyond quarterly earnings.
Apollo's journey from one 150-bed hospital to Asia's healthcare giant isn't just a business success story. It's validation that emerging markets can build world-class institutions. It's proof that family businesses can professionalize without losing their soul. And it's evidence that in healthcare, quality and scale aren't trade-offs—they're complementary.
For investors, Apollo represents a unique opportunity to participate in India's healthcare transformation. The company combines the stability of an established leader with the growth potential of emerging businesses. As India's middle class expands and healthcare consumption increases, Apollo is positioned to capture a disproportionate share of value creation.
The story that began with a letter from a father to his son has become the story of Indian healthcare itself. And it's far from over.
 RSS Feed
RSS Feed Spotify
Spotify Apple Podcasts
Apple Podcasts Amazon Music
Amazon Music Audible
Audible YouTube
YouTube